Manual Wheelchair User Hand Force Measurement In The Field: A Preliminary Report
Melissa M.B. Morrow, Meegan P. Van Straaten, Kristin D. Zhao, Beth A. Cloud, and Kenton R. Kaufman
Division of Orthopedic Research, Mayo Clinic, Rochester, MN
Abstract
Manual wheelchair users are at a high risk for upper extremity pain and injury due to their reliance on their arms for mobility. Kinematics and kinetics of activities of daily living performed by manual wheelchair users have been studied to determine a link between applied forces and motion with pain. However, data collected in the laboratory only captures isolated tasks that may not represent the loads and motion in the field. The purpose of this preliminary report was to document the validation and first use of a prototype forceglove for measuring hand forces in the real world environment in manual wheelchair users. The forceglove was successfully used to collect preliminary data from 7 participants. Results suggest that the majority of the forces experienced during the day were of low magnitude with infrequent, singular high load events, but it is yet to be seen if this trend will be consistent among a larger sample of manual wheelchair users.
Background
Individuals with spinal cord injury often use manual wheelchairs as their primary mode of mobility, and thus, utilize their upper extremities for all recreational and professional activities of daily living (ADLs). The joint geometry of the upper extremity is poorly designed for weight bearing (Requejo & Mulrouy, 2008) and its musculature is smaller and less efficient for ambulating as compared to the large musculature of the lower extremity. This places manual wheelchair users at a high risk of upper extremity pain and injury, limiting not only their mobility, but all ADLs (Bayley, Cochran, & Sledge, 1987). Injury and subsequent loss of function have major ramifications for quality of life and places a large economic burden on the individual and associated health care systems (French et al., 2007). Prevention of upper extremity pain and injury can help manual wheelchair users avoid further disability and the costs required for proper treatment.
Before a focused prevention protocol can be prescribed, a link between injury resulting from modifiable risk factors and the activities that contribute to that injury must be determined. Although much progress has been made into upper extremity dysfunction prevention, previous work largely used handrim kinetics as a primary outcome measure, and inferences about injury mechanisms were made based on level propulsion laboratory experiments alone (Boninger, Baldwin, Cooper, Koontz, & Chan, 2000). Research in our laboratory has shown that laboratory data collection is not a surrogate for real-world wheelchair propulsion (Hurd, Morrow, Kaufman, & An, 2008), and collecting data in the field, or in the natural environment, is necessary to fully characterize actual demands that are put on the upper extremity of manual wheelchair users.
purpose
The overall objective of this line of research is to link shoulder pain and injury in manual wheelchair users with the kinematics and kinetics of their ADLs as measured in the field. The purpose of this preliminary report is to document the validation and first use of a prototype forceglove for measuring hand forces in the real world environment.
methods
Study Participants
Twenty adults were recruited and consented for participation in the IRB approved study, and 7 participants completed testing (40±9 years, 77±20 kg, Table 1). For inclusion in the study, participants were required to be between 18 and 65 years of age, manual wheelchair users for at least six months prior to the study, have full active upper extremity range of motion, and strength of 4/5 as measured with manual muscle testing throughout the upper extremity.
| Subject | Age (yrs) | Weight (kg) | Injury level | WC use (yrs) | Transfer (#) | WUSPI score | Max force (N) |
|---|---|---|---|---|---|---|---|
1 |
33 |
116 |
T5 |
10 |
13 |
16.0 |
165.2 |
2 |
28 |
78 |
T10/11 |
10 |
15 |
22.3 |
255.6 |
3 |
36 |
83 |
Spina bifida |
36 |
10 |
0.0 |
133.6 |
4 |
35 |
50 |
T4/5 |
19 |
8 |
6.4 |
112.9 |
5 |
51 |
64 |
Trans myelitis |
13 |
10 |
69.4 |
94.7 |
6 |
46 |
72 |
T12 |
5 |
14 |
8.4 |
75.7 |
7 |
48 |
75 |
T4 |
17 |
11 |
1.4 |
113.6 |
Physical Exam
A physical exam was performed on all study participants by a licensed physical therapist. The participant’s range of motion of the upper extremity and trunk; joint integrity of the shoulder, elbow and wrist; trunk stability; and strength were evaluated. In addition, age, gender, injury level, hand dominance, years of wheelchair experience and history of upper extremity injury or complaints of pain were documented.
Forceglove Validation
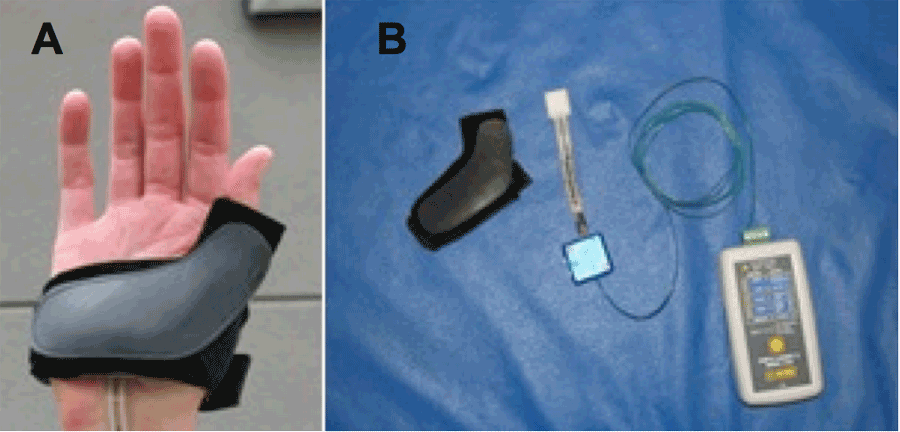 Figure 1: Custom-built forceglove on the hand (A), force glove components (B)
Figure 1: Custom-built forceglove on the hand (A), force glove components (B)Prior to participant testing, a custom-built prototype forceglove (Fig 1) was developed and validated in the laboratory environment. The force glove consisted of the glove, FlexiForce sensor (Tekscan), electronics, and data logger (Track-It). The FlexiForce sensor is centered on the proximal palmar surface of the hand within a metal cage, beneath the glove exterior, and the remaining electronics were attached to the arm. The validation procedure used a table-embedded forceplate (AMTI) and a Smartwheel instrumented wheelchair handrim (Three Rivers). On the forceplate, a sit-and-pivot transfer was performed with the forceglove on the leading hand. Loading during wheelchair propulsion and a weight relief maneuver were tested with the Smartwheel handrim. Data from the forceglove were collected at 4 samples per second.
Field Collection
Prior to field collection, each forceglove was calibrated using a 5-point, static load linear calibration. The field collection consisted of collecting kinematics and kinetics for one typical day in the user’s natural environment. At the start of the field collection, the participant completed a Wheelchair User’s Pain Index (WUSPI) questionnaire (Curtis et al., 1995). The participant donned the forceglove on the hand of the limb with the most painful shoulder. The collections were scheduled to last for 8 hours, participants recorded the number of transfers performed, and no study staff were present after equipment set-up.
Analysis
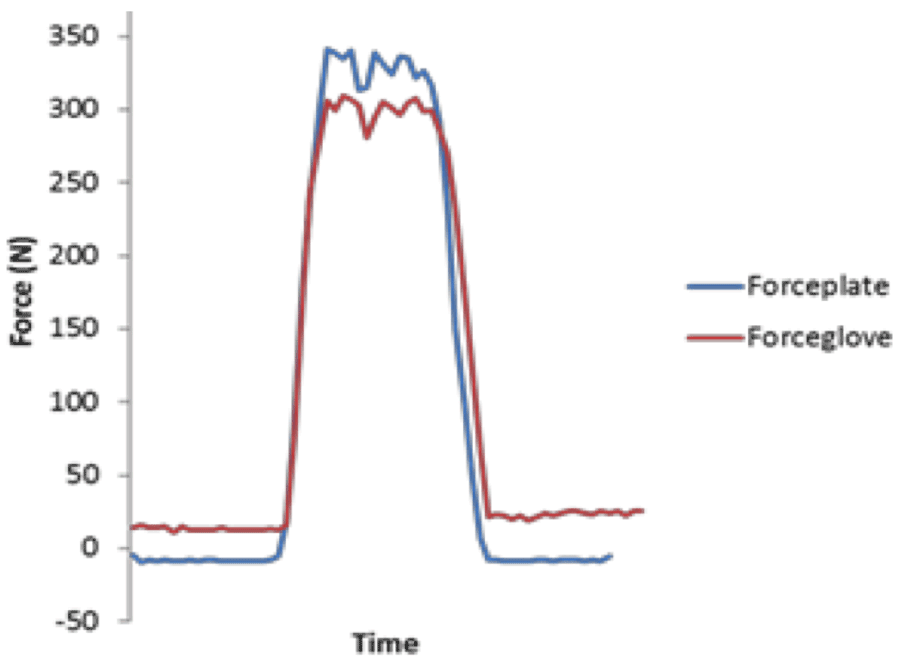 Figure 2: Sit-and-pivot transfer force measuresment of the leading hand with forceplate and forceglove
Figure 2: Sit-and-pivot transfer force measuresment of the leading hand with forceplate and forceglovePreliminary forceglove data were available on 7 participants for analysis. The force data were expressed in Newtons and the maximum measured force was determined for each subject. The force magnitudes below 1N were classified as zero or no force meaning there was no loading on the glove. The remaining measured forces over the entire day were divided into 3 equally-divided quantiles representing low, medium and high forces. The percentage of the measured forces in each quantile was determined for each particpant. Additionally, qualitative observations were made in the relationship between the force data and the WUSPI questionnaires.
results
Study Participants
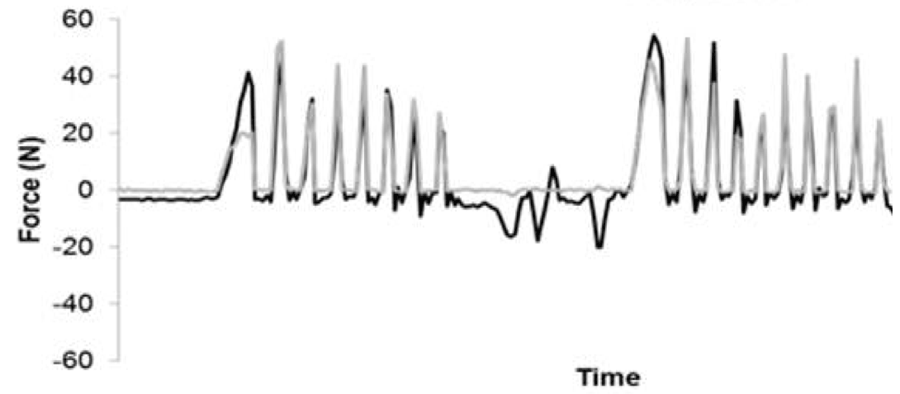 Figure 3: Level wheelchair propulsion measured with both a Smartwheel rim (black line) and forceglove (grey overlaid line).
Figure 3: Level wheelchair propulsion measured with both a Smartwheel rim (black line) and forceglove (grey overlaid line).Five out of the 7 participants who have completed testing suffered traumatic spinal cord injuries (Table 1). On average, the participants have used manual wheelchairs for 16 years. On the day of the field collection, participants averaged 12 transfers and scored between 0 and 70 out of 150 on the WUSPI questionnaire (Table 1). Zero indicates no pain while a high score indicates more pain.
Validation
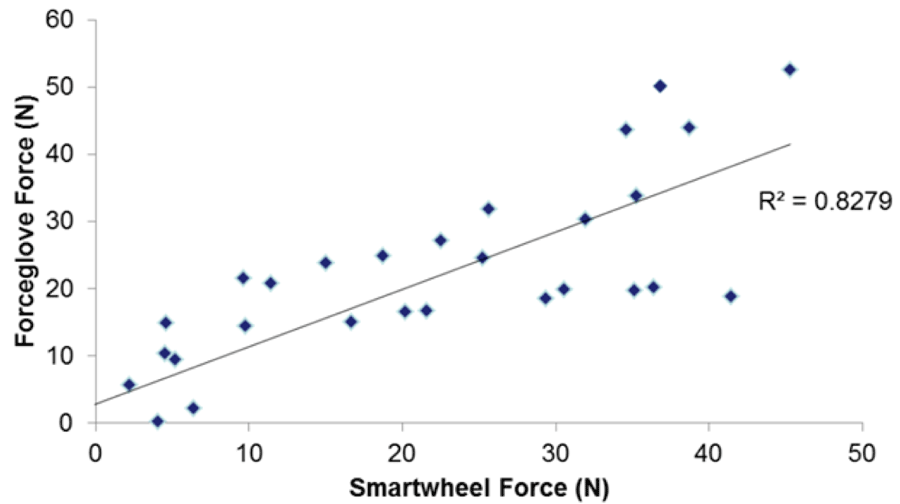 Figure 4: Correlation of forces measured by the Smartwheel rim and the forceglove
Figure 4: Correlation of forces measured by the Smartwheel rim and the forcegloveThe forceglove showed good qualitative agreement with the forceplate during the sit-and-pivot transfer (Fig. 2) in addition to during wheelchair propulsion (Fig. 3). A regression between the forceglove output and the Smartwheel forces during wheelchair propulsion showed an R2 value of 0.83 (Fig. 4).
Field Collection
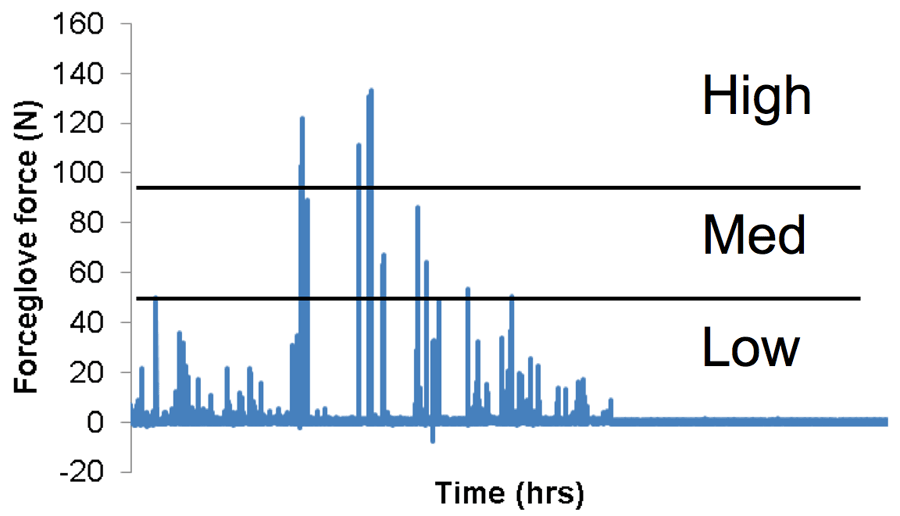 Figure 5: Representative forceglove time series data from one full day collection from participant 3. The 3 quantiles are labeled as high, moderate (med), and low force magnitudes.
Figure 5: Representative forceglove time series data from one full day collection from participant 3. The 3 quantiles are labeled as high, moderate (med), and low force magnitudes.A range of forces was measured in the field during the day long collection (Fig. 5), and the maximum recorded forces ranged from 76N to 256N (Table 1). The majority of the data registered by the forceglove showed little to no loading of the glove during the day (Table 2) with less than 1% of the day spent in the medium or high force quantiles. Qualitatively, participant 3, with the lowest WUSPI score (no pain), experienced the least percentage of the day in the no force category and participant 5, with the highest WUSPI score (more pain), experienced the highest percentage of the day in the no force category (Table 2). Participant 5 may have been performing less loading activities to avoid shoulder pain.
Figure 5: Representative forceglove time series data from one full day collection from participant 3. The 3 quantiles are labeled as high, moderate (med), and low force magnitudes.
Subject |
No Force (%) |
Low Force (%) |
Medium Force (%) |
High Force (%) |
1 |
89.20 |
10.60 |
0.1 |
0.09 |
2 |
99.40 |
0.50 |
0.03 |
0.06 |
3 |
87.20 |
12.69 |
0.08 |
0.04 |
4 |
91.99 |
7.93 |
0.07 |
0.01 |
5 |
99.70 |
0.26 |
0.01 |
0.03 |
6 |
98.59 |
1.38 |
0.02 |
0.01 |
7 |
96.03 |
3.73 |
0.22 |
0.02 |
discussion
The prototype forceglove was successfully validated and was shown to measure a range of forces in the field at the proximal palmar region of the hand. This study represents a proof-of-concept that kinetic data, traditionally only collected in the laboratory setting, can be collected in the field in the user’s natural environment.
The majority of the day for the 7 tested participants was spent without any loading on the forceglove (Table 2). This more than likely represents a combination of (1) the actual low occurrence of loading on the palmar surface of the hand with (2) loading that did not engage the FlexiForce sensor. The magnitude of forces typically measured during level wheelchair propulsion using an instrumented handrim fell into the low to medium force category for most of the participants, but it remains to be seen if the percentages of low force measured in this study are representative of a typical manual wheelchair user. For example, participant 4 spent nearly 8% of a 9 hour day in the low force range which could potentially account for roughly 45 minutes of propelling. After further analysis is performed on the data to identify specific activities, more thoughtful conclusions can be made.
This study had some limitations. Adequate measurement of hand forces requires that the participant load the hand directly over the force sensing area. This likely resulted in an underestimation of the magnitude and frequency of forces experienced in the field. The sampling rate of the data logger was only 4 samples/sec which may have caused loading events to be missed. Additionally, these data only represent one day of the participant’s life and may not have been representative of their typical loading magnitudes and rates.
Conclusion
A custom, prototype forceglove was successfully validated and used in manual wheelchair users to collect hand forces in the field during a typical day. The preliminary data suggested that the majority of the forces experienced during the day were of low magnitude with infrequent, singular high load events, but it is yet to be seen if this trend will be consistent among all 20 participants.References
Acknowledgements
Funding for this project was provided by the Paralyzed Veterans of American Foundation.